By clicking “Accept,” you agree to the use of cookies and similar technologies on your device as set forth in our Cookie Policy and our Privacy Policy. Please note that certain cookies are essential for this website to function properly and do not require user consent to be deployed.
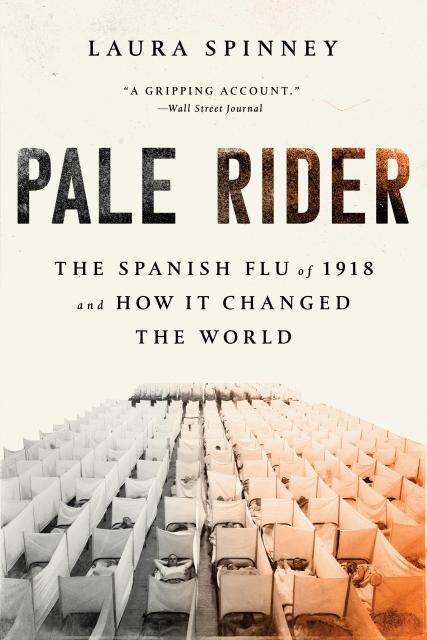
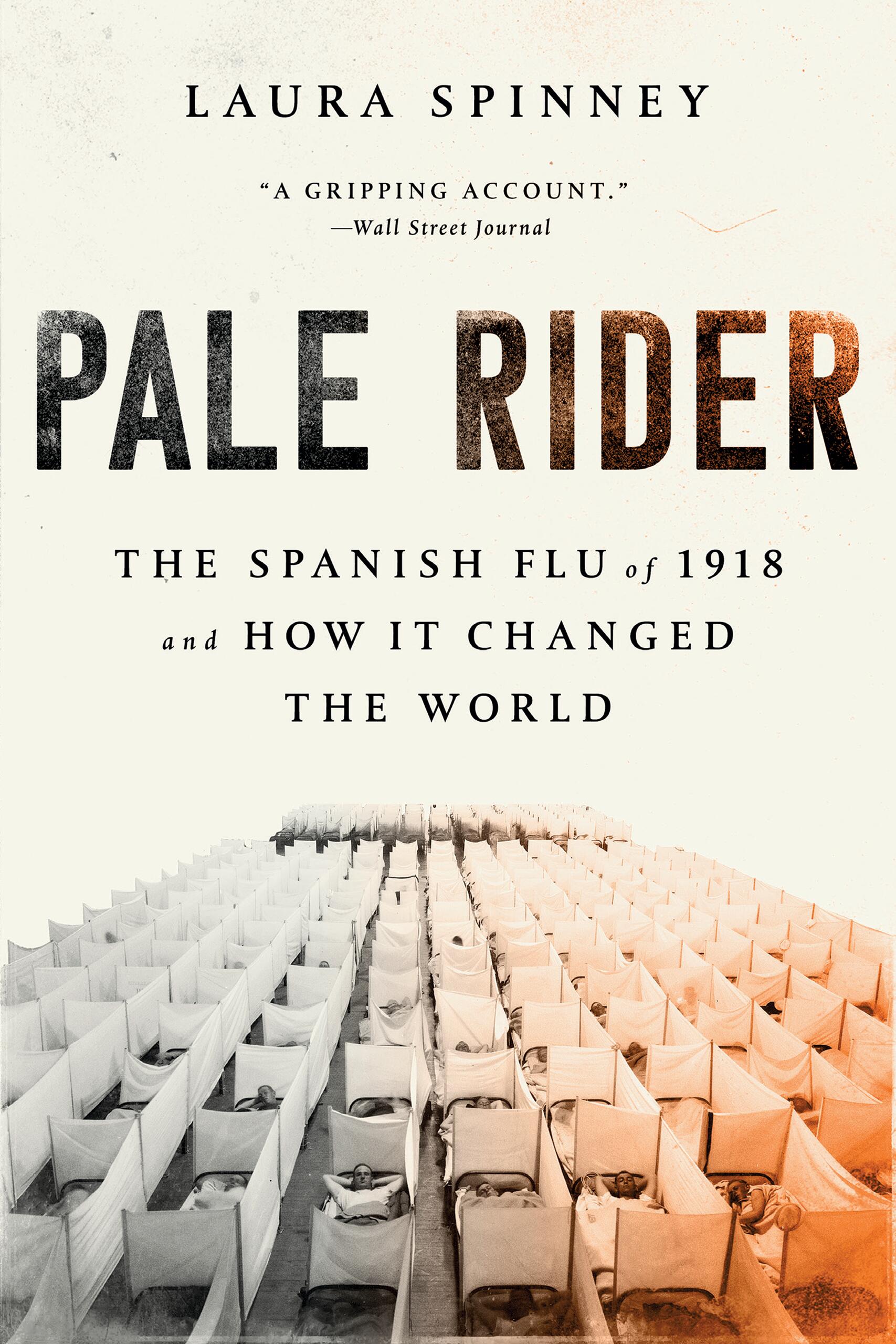
Pale Rider
The Spanish Flu of 1918 and How It Changed the World
Contributors
Formats and Prices
- On Sale
- Sep 18, 2018
- Page Count
- 352 pages
- Publisher
- PublicAffairs
- ISBN-13
- 9781541736122
Price
$19.99Format
Format:
- Trade Paperback $19.99
- ebook $12.99
- Audiobook Download (Unabridged)
- Trade Paperback (Revised) $21.99 $28.99 CAD
This item is a preorder. Your payment method will be charged immediately, and the product is expected to ship on or around September 18, 2018. This date is subject to change due to shipping delays beyond our control.
Buy from Other Retailers:
The haunting story of a virus that triggered the worst pandemic of modern times.
“Both a saga of tragedies and a detective story.” —The Guardian
The flu pandemic of 1918–1920 was one of the greatest human disasters of all time. It infected a third of the people on Earth—from the poorest immigrants of New York City to the king of Spain, Franz Kafka, Mahatma Gandhi, and Woodrow Wilson. But despite a death toll far higher than that of World War I, the 1918 flu is little more than a historical afterthought.
In this gripping narrative history, Laura Spinney reveals how the virus traveled across the globe, exposing humanity’s vulnerability and putting our ingenuity to the test. She demonstrates how the 1918 flu shaped the modern world by disrupting, and often permanently altering, global politics, race relations, and family structures.
Now with a new afterword reflecting on the impacts of COVID-19, Pale Rider is a masterful account of the catastrophe that forever changed humanity.
-
“A gripping account... A cautionary tale about human vulnerability and ingenuity in the face of peril.”The Wall Street Journal
-
“Impressive… Set against the devastating backdrop of global contagion, it is individual lives and deaths, discovered in letters, diaries, biographies and memoirs, that epitomize this rich account. Spinney invokes potent images… Along with exemplary research, Spinney’s narrative is packed with fascinating, quirky detail… As the centenary of this monumental event approaches, other volumes on the pandemic will undoubtedly appear. Pale Rider sets the bar very high.”Nature
-
“Both a saga of tragedies and a detective story… Pale Rider is not just an excavation but a reimagining of the past. As the book progresses, the flu is cast increasingly as a character that crops up Zelig‑like at important moments in history, altering the course of events previously unattributed to it.... Compelling.”The Guardian
-
“A book about the Spanish flu could so easily be dreary—complex pathology interwoven with pervasive tragedy. Not so Pale Rider. I’ve seldom had so much fun reading about people dying. Laura Spinney, a science journalist, is adept at explaining arcane scientific research in an entertaining, comprehensible way… With superb investigative skill and a delightfully light‑hearted writing style, Spinney extends her analysis far beyond the relatively short duration of the plague… Spinney finds it odd that we know so little about the worst calamity to affect the human race. So do I. There are tens of thousands of books about the First World War, yet that flu is, arguably, more relevant to our world. While global war is, we hope, a thing of the past, global pestilence hovers like a vulture.”The Times (UK)
-
“Spinney argues that almost a century later, the Spanish flu is ‘still emerging from the shadows of the First World War’ in our collective memories. She sets out to rectify this, knowing just which medical mysteries and haunting vignettes will give the pandemic full purchase on our imaginations.”The New York Times
-
“Wide‑sweeping… Spinney is a storyteller with a science writer’s cabinet of facts. Retracing influenza’s death trail over nine continents, she attempts to show how the flu affected not only the war‑torn West but also remote communities in South Africa, China, and Brazil. The book reveals how desperately and differently people reacted and how gravely the flu influenced the modern world, touching everything from medicine to business and from politics to poetry.”Science
-
“Influenza, like all viruses, is a parasite. Laura Spinney traces its long shadow over human history… Ms. Spinney ties the virulence of Spanish flu to its genetic irregularities and does a good job of explaining containment strategies through epidemiology… In Europe and North America the first world war killed more than Spanish flu; everywhere else the reverse is true. Yet most narratives focus on the West… Ms. Spinney’s book goes some way to redress the balance.”The Economist
-
“Weaves together global history and medical science to great effect… This riveting study plots the course of the deadliest pandemic in history.”The Sunday Times
-
“Ambitious… Spinney delves into the unfolding tragedy around the globe, looking at Brazil, China, Iran, India, and Russia. There is fascinating detail.”Spectator
-
“An excruciating report on the global disaster… Absorbing… Spinney’s important book does not attempt to offer light reading. No less than four pandemics are predicted in the 21st century. At least one will take the form of flu. Vaccination is not cheap, because the flu virus is constantly mutating. Annual vaccines currently offer the best protection. Britain does still possess a National Health Service. The enduring message of Spinney’s magisterial work is to underline just how crucial that remarkable service is to the future security of an unusually privileged nation. Let's hope the author’s book is read with care by Theresa May.”The Observer
-
“Spinney’s book is intensely readable, and instead of a strictly chronological account she circles around history, epidemiology and culture to give a panoramic portrait of the previous century’s most deadly pandemic. We are probably due another one of these any day now, this is a great way to see what the future holds.”The Awl
-
“A page turner that should easily satisfy armchair historians and epidemiologists and anybody who likes a good, if gruesome, yarn.”Foreign Policy
-
“A masterful account of the possible origins, spread, and cultural consequences of this modern‑day plague.”Geographical
-
“A vividly recreated, grimly fascinating book… Coolly, crisply and with a consistently sharp eye for the telling anecdote… Spinney demonstrates how Spanish flu cast a long, dark shadow over the 20th century.”The Daily Mail
-
“[Spinney] evokes a world that seems both farther from us than a mere century, and also uncomfortably close… If we can’t reconstruct our memories of the Spanish flu quickly enough, millions more will die in the next pandemic.”The Tyee
-
“Remarkable… a concise but comprehensive work.”The Cascadia Advocate
-
“One of the many strengths of Pale Rider is to show its readers the regional variations that combat took throughout the world, from Bristol Bay to Zamora to Unalaska Island… For all the tragedies and upheavals, the book portrays, Pale Rider actually paints an oddly hopeful picture of a population more sensitized to early warnings and largely more willing to heed them.”The National
-
“Scarier than science fiction… You’ll want to get your flu shot after reading this book.”Zócalo
-
“A frightening new book… Those readers wishing to prevent tragedies like the one in 1918 should read this book.”Lincoln Journal Star
-
“An insightful and valuable account for all history collections.”Library Journal
-
“A compelling, expert account of a half‑forgotten historical catastrophe.”Kirkus
-
“Pale Rider contains vivid journalistic accounts of outbreaks around the world, from the U.S. to China, India, and Persia...Insightful.”Publishers Weekly
-
“Spinney's detailed discussion includes the why and how, the human devastation, and the effects on institutions and world affairs. Now nearly 100 years removed from the 1918 Spanish flu, Spinney wonders what lessons it has imparted that might help us prepare for and deal with the next, inevitable influenza pandemic.”Booklist